
Sacro-Iliac Joint
Mr Khitish MohantyConsultant Trauma & Orthopaedic Surgeon, UK
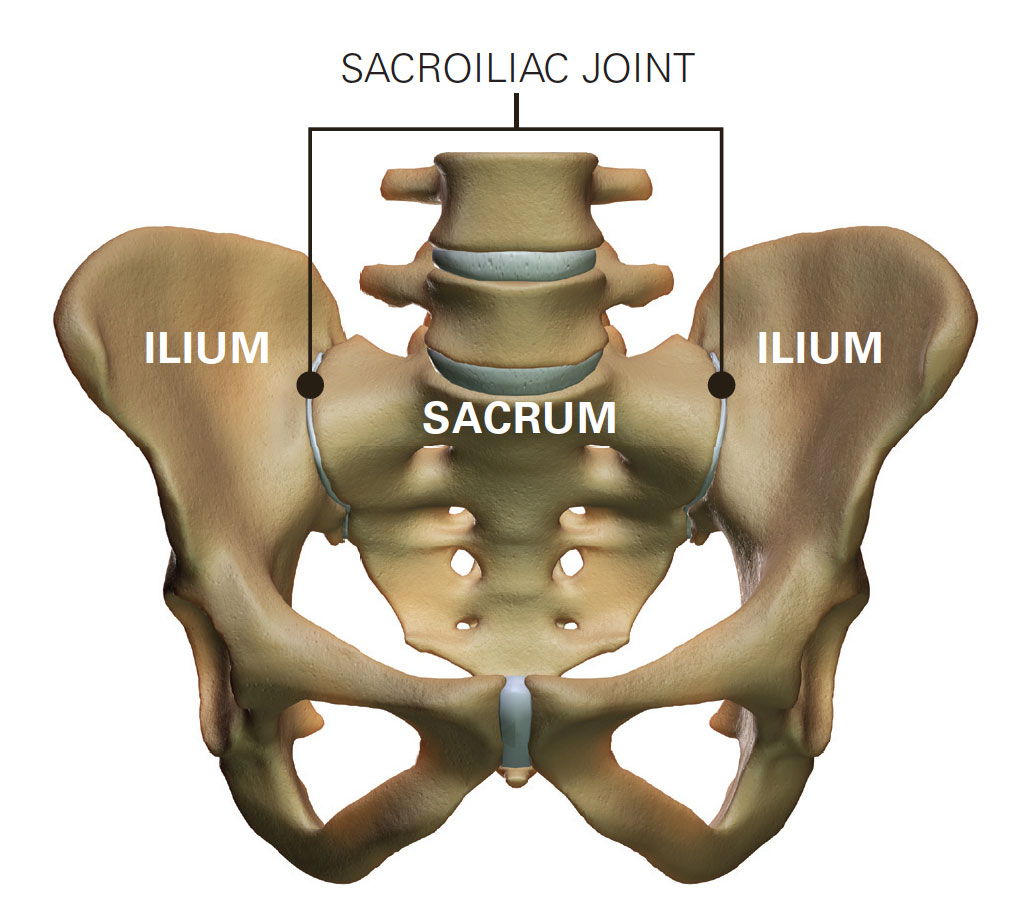
Sacroiliac joint is a pair of special joints located between the lower back and the hip joint. Although they move a few degrees during normal locomotion they are critical in weight transfer and are two weight bearing joints. These joints get loaded particularly at the time of sitting and negotiating gradient.
The importance of a sacroiliac joint as the cause of low back pain has been highlighted in recent medical literature.
Studies have shown that up to 25% (a quarter) of low back pain could be attributed to the sacroiliac joint.
Causes of Sacro-Iliac Joint Pain
Sacroiliac joints, being a synovial joint, can get affected by any arthritic condition which affects the other joints like the hips and knees. These conditions include osteoarthritis, rheumatoid arthritis, gout, ankylosing spondylitis etc. Sacroiliac joint can also get affected by post-pregnancy instability and subtle injury to pelvis during difficult childbirth. Sacroiliac joint dysfunction is also quite common secondary to blunt injury to the pelvis and low back particularly due to mechanical fall. These joints can also become painful following secondary involvement and arthritis following high velocity pelvic ring injuries. More recently, sacroiliac joint problems have been identified to be caused by previous hip operation, particularly fusion of the lower lumbar spine due to secondary stress transfer.

Symptoms
Patient’s with sacroiliac joint disorder present with either uni-lateral (one-sided) or bi-lateral (both sided) low back and buttock pain. Typically the pain radiates to the thighs up to the knee and can also radiate to the groin, hip and lower abdomen. It is unusual for sacroiliac joint pain to radiate below the knee and it is usually not associated with tingling and numbness in the feet. Typically patients with sacroiliac joint dysfunction would struggle to sit square on a firm surface and would fidget around as they are not able to load the affected sacroiliac joint. They would also find it difficult to turn in bed and negotiate gradient and climb stairs. In advance cases patients with sacroiliac joint disorder would find it very difficult to walk unassisted and they would have to rely on crutches or a wheelchair.

Clinical Assessment and Diagnosis
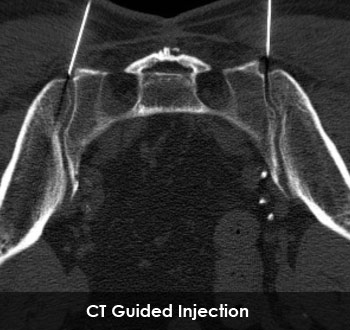
It is difficult to isolate sacroiliac joint pain from pain arising from the lower lumbar spine particularly due to the close proximity of the two structures. After a careful history, clinical examination and provocative tests, various investigations like plain x-ray and MRI scan are carried out. These investigations although not diagnostic of sacroiliac joint conditions, help to rule out all other pathology around that area. The accurate diagnosis of sacroiliac joint dysfunction relies on an image guided injection of local anaesthetic to the suspected sacroiliac joint. These injections can be done either under CT scan guidance or fluoroscopic control. Positive response of pain relief following an image guided injection leads to the diagnosis of sacroiliac joint dysfunction.

Management
After a firm diagnosis is established, sacroiliac joint disorder is treated initially conservatively with a focused programme of physiotherapy and rehabilitation aided by anti-inflammatory and other medications. Other modalities of treatment like acupuncture, prolotherapy and chiropractic therapy along with manipulation have also been advocated for this condition.
Surgical Treatment
Open operation and fusion of the sacroiliac joint is not very popular. The historical studies have shown high rates of wound complication, infection and operation related morbidity due to the location of the joint. Over the last five to six years there is an impetus on percutaneous stabilisation/fusion of the sacroiliac joints. The percutaneous fusion is done through a keyhole method under image guidance and patients typically spend one night in hospital. Mr Mohanty has pioneered percutaneous sacroiliac joint stabilisation for various sacroiliac joint conditions in the UK (see Clinical Practice and Publication section).
Post-Operative Management
Patients are discharged from hospital the day after the percutaneous keyhole sacroiliac joint stabilisation. Patients are allowed to walk partial weight bearing with the help of crutches for up to four to six weeks. In approximately six weeks from the date of the operation patients are allowed to mobilise independently. A course of post-operative physiotherapy is included in the care package.
Result
In a carefully chosen patient’s group, where a firm diagnosis of sacroiliac joint dysfunction has been established, keyhole stabilisation of the sacroiliac joint has been shown to produce effective and sustained pain relief and relief of symptoms. Mr Mohanty has presented his results in various peer reviewed society and also published his results in peer reviewed journals such as Journal of Bone and Joint Surgery and European Spine Journal (see Publication). Mr Mohanty continues to carry out prospective research study on all patients having this novel but revolutionary procedure.
Complications
Although this procedure is generally safe and the majority of people do very well there is the potential for nerve injury particularly to the sacral nerve root following this percutaneous procedure.
A minority of patients also complain of persistent pain in their lower back following this procedure.
Patient’s Story
Overlooked Cause of Low Back Pain: The SI Joint with Mr Khitish Mohanty